 Content creation considerations for 3D models destined for augmented and virtual reality also exist, and they are primarily driven by the computational requirements of rendering images and the computational ability of a given system. For VR, computers have to render images for two HD displays, one for each eye, with both displaying data in a synchronized manner at a high frame-rate (typically greater than or equal to 72 Hz). This can impose constraints on the total number of triangles that can exist in a given scene to be rendered, but with today’s high-powered graphics cards, this constraint is rarely a limitation.
Content creation considerations for 3D models destined for augmented and virtual reality also exist, and they are primarily driven by the computational requirements of rendering images and the computational ability of a given system. For VR, computers have to render images for two HD displays, one for each eye, with both displaying data in a synchronized manner at a high frame-rate (typically greater than or equal to 72 Hz). This can impose constraints on the total number of triangles that can exist in a given scene to be rendered, but with today’s high-powered graphics cards, this constraint is rarely a limitation.
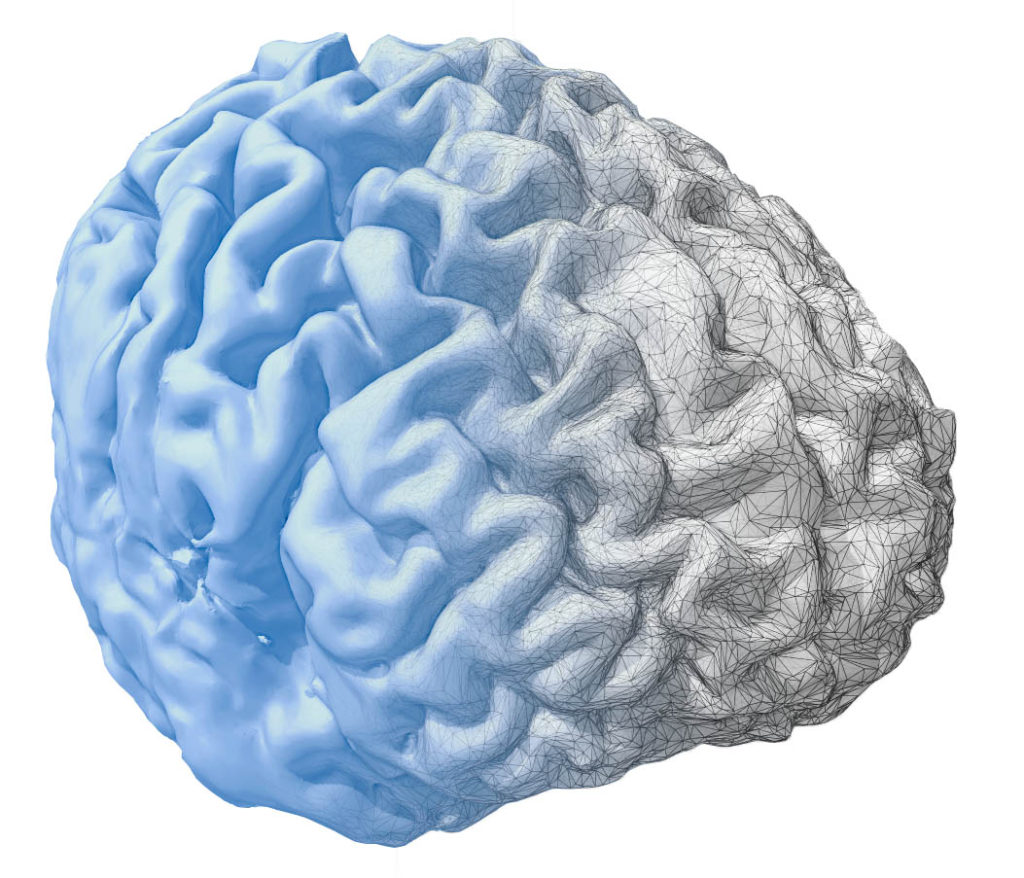
Mobile mixed reality devices, however, often have a significantly reduced computational ability and, as such, have more strict constraints on the number of triangles that can be rendered in a given scene. This can potentially create a challenge for model creators that need include enough detail to maintain anatomic fidelity while also avoiding models that have become ‘dis-featured’ due to exceeding model size limitations. In most mobile-use cases currently, the number of triangles in meshes can be reduced through decimation to accommodate rendering constraints. However, fully-detailed models should soon be widely accessible to mobile platforms through the a growing number of cloud-rendering services where images are rendered remotely by high-powered systems and served in real-time to mixed reality displays through Wi-Fi or 5G networks.